×

The Standard e-Paper
Smart Minds Choose Us
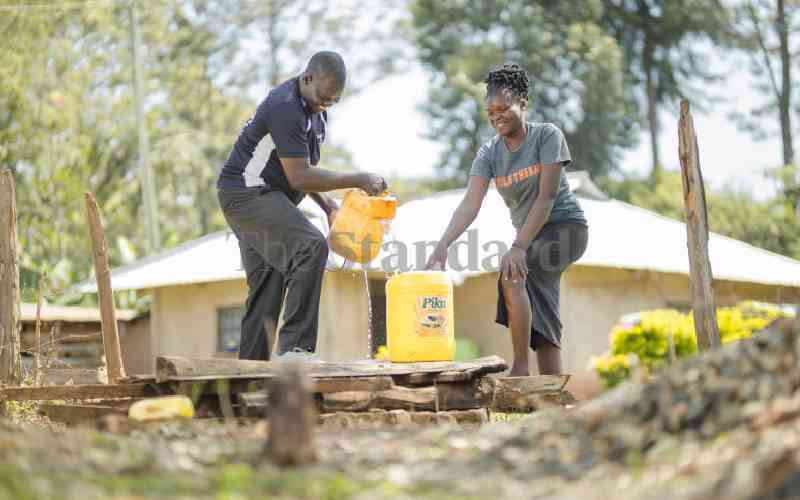
When numbers about health are thrown around at community gatherings that he attends in K'akrao in Migori County, John Mbago's heart skips a beat due to fear. One in five girls under 18 years old (22 per cent) are already teen mothers, according to the latest Kenya Demographic Health Survey.
About 14.7 per cent of the population is living with HIV, the fourth highest in Kenya, according to data from National Aids and STIs Control Programme (Nascop). There are more than 8,000 new HIV infections in Migori each year.
Subscribe to our newsletter and stay updated on the latest developments and special offers!