×

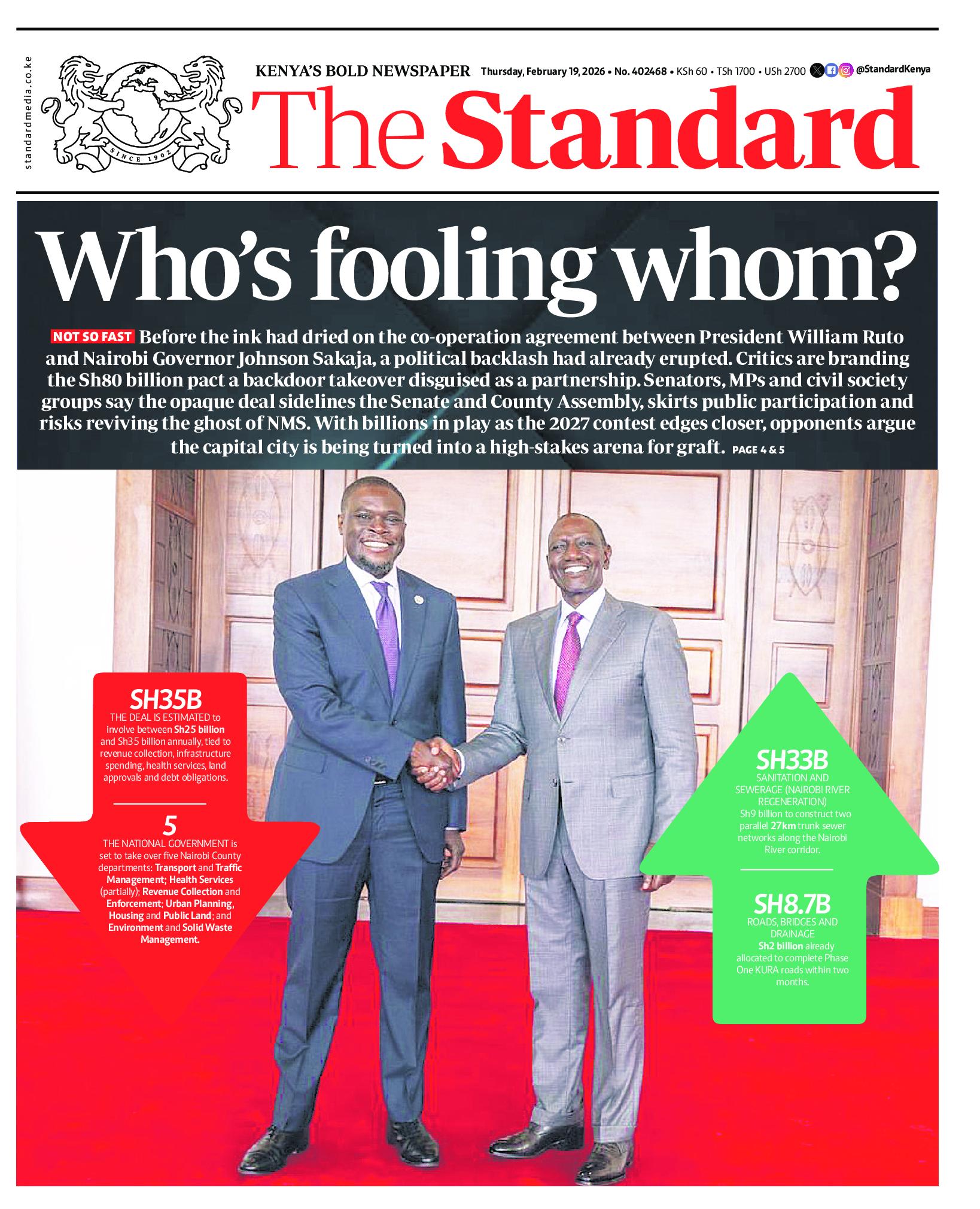
The Standard e-Paper
Join Thousands Daily







Subscribe to our newsletter and stay updated on the latest developments and special offers!