The Standard Group Plc is a
multi-media organization with investments in media platforms spanning newspaper
print operations, television, radio broadcasting, digital and online services. The
Standard Group is recognized as a leading multi-media house in Kenya with a key
influence in matters of national and international interest.
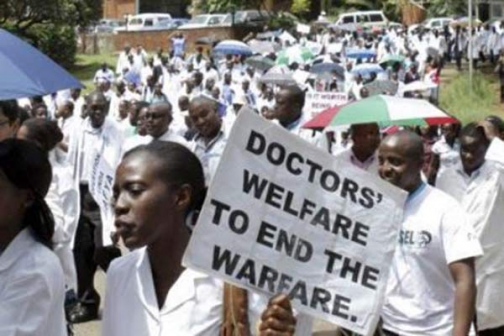
Many doctors and patients are cognizant of the fact that locally, the national rationale of only responding to patient or worker complaints during crisis thrives even in private facilities. Further to this, prices and qualities of care vary so widely between facilities and service providers that it is difficult to reliably project treatment costs, especially in the case of chronic conditions.PHOTO:COURTESY
The nation spends a lot of time bemoaning the brains that carry our best minds and talents away from the public health sector.
Eighty per cent of Kenyan doctors reportedly leave the civil service either for private practice locally or across the borders to work for public or private health care sectors abroad. This means that for every five doctors trained in Kenya, the public sector is only able to retain one despite the urgent need for trained personnel.
This is remarkably similar to the exodus of talent that we see in sports—we are accustomed to celebrating excellence by familiar names competing under the flags of strangers.
The ethics are of course murky— we are happy for Kenyans to use every chance they can to grow professionally and to be well remunerated, and yet we are still left with unfair, if legitimate, questions about patriotism and about who will fix the systems we all know are deeply broken if everybody leaves. The nation remains in a crisis point, with our doctors remaining steadfast in the strike for better care for all Kenyans.
Meanwhile, it is important that we start reflecting about alternative solutions and understand how the fight for universal healthcare has worked out in countries that bear more similarities to ours than those in the global North. It is all very well and good to aspire to European, American or Australian standards, but we cannot compare our economic and social contexts to theirs, and must look closer to home for solutions that have any true potential.
Senior civil servants in the Ministry of Health have been quoted as saying that they are ready to hire doctors from India to replace our own in the civil service. This is stated in a manner to suggest that they can carry over some public service excellence to better serve the people of Kenya. Perhaps we should have a more nuanced understanding of how public health in India works, and the short version of that discussion is: It doesn’t.
India has the second largest population in the world, coming up at just under 1.3 billion people and growing every day, but has under half the doctors a population that size would need to service its health needs. The services that the world seeks via their thriving medical tourism industry are priced at roughly 10 per cent of the cost in UK and US hospitals, which may sound reasonable and affordable from afar.
However, these same services are offered by mostly urban, private healthcare providers, and are therefore only available to the rich and middle class even locally. The description of their available conveniences, such as reduced waiting time, access to the most advanced, highest quality investigations and procedures, or treatment of complicated conditions, scream “market” long before they hint at any forceful, effective public policy.
Let us recall that the vast majority of the population (just under 70 per cent) live in rural areas, with just about a quarter of the billion plus eking out survival under the poverty line of a dollar and a quarter a day. Perhaps they have fantastic health insurance policies, one might hope? Not quite: just under 20 per cent of the population is covered by any kind of health insurance.
The vast majority of Indians have to pay for any health services directly out of pocket, many selling assets or borrowing to meet unexpected expenses, and many others relying on homeopathic remedies despite the fact that lower cost generic drugs are widely available in the country. Kenya has almost identical statistics.
We also have under half the doctors needed for our population of over 45 million. The best quality care is also located in urban areas, excluding the 75 per cent of rural citizens. Just over 20 per cent of our population has some manner of health insurance, whether public via the National Health Insurance Fund (NHIF), or from a for-profit corporate.
Unanswered questions continue to be asked of NHIF about their willingness to fork out taxpayer funds to pay private facilities or even Indian hospitals to treat Kenyans, rather than engage in any meaningful dialogue to improve care in government facilities.
There are clearly flaming ethical considerations in making any kind of arrangement with the Indian government to hire doctors for ourselves from them, when they remain so sorely in need of their own. Individual doctors are, of course, free to work wherever they may choose.
In any case, we seem to be having deepening discussions with the Indian government ostensibly about strategies to improve our healthcare sector and become a medical tourism destination, when they gave up the battle for public healthcare in their own home decades ago and instead have refined a market-based approach to the clear detriment of the majority of citizens.
The mere fact that we look to them as any kind of example with regard to universal healthcare is not only troubling but deeply hypocritical.
Stay informed. Subscribe to our newsletter
Another place touted as a source of doctors for Kenya is Cuba, and it is important to understand how things work there as well. Until the socialist revolution in 1959 which brought the late Fidel Castro to power, Cuba ran the same vaguely hybrid system of private/public healthcare that is familiar worldwide. After the revolution, things drastically changed.
Pushed by Castro, the Cuba government began to deliver free universal healthcare at all levels. Diseases that would cost thousands of dollars to manage in the nearby United States are treated free of charge. Further to this, the country’s sharp focus on disease prevention over cure led to community-oriented medicine, with care providers integrating outpatient home visits and follow-ups into hospital investigations and inpatient management.
Cuba’s doctors and their healthcare system also face challenges. The long US embargo, only recently lifted, made it incredibly difficult for Cuba to renovate and update its medical equipment, and doctors have long complained about limited access to modern treatment facilities. When Cuban doctors leave their homes to work elsewhere, those left holding the fort are overworked and overstretched.
Additionally, the Cuban government profits when its doctors are posted elsewhere, in their role as Cuba’s most valuable export, to the tune of billions of dollars annually.
There are ethical questions in taking advantage of a situation like that, excellent as Cuba’s care workers may be. Additionally, even if Cuban doctors joined our civil service, it would be impossible for us to mirror the exact community care frame that enables them to be such stellar caregivers.
Finally, if one day public health services in this country suddenly collapsed irreversibly and left the local private care sector to step up to the plate one hundred per cent, we would still have many issues. Kenyans have learned to associate private service provision with high quality, and this association is not always true.
Many doctors and patients are cognizant of the fact that locally, the national rationale of only responding to patient or worker complaints during crisis thrives even in private facilities. Further to this, prices and qualities of care vary so widely between facilities and service providers that it is difficult to reliably project treatment costs, especially in the case of chronic conditions.
Moreover, private insurers, who have remained uncritiqued due to their tiny local market share, often omit to educate patients on important fine print exceptions and limits in their policies. This leads to unexpected out of pocket costs even to people who are already paying to be covered.
NHIF spending would need to be radically revised to accommodate the entire population of 45 million Kenyans registering at private facilities (which make up 43 per cent of all health facilities nationally), which clearly do not have the capacity to cater for us all. Without a serious long term strategy, therefore, it is not difficult to imagine a point in time where Kenyans are fundraising to cater for absolute basics like the treatment of diarrhoea and malaria for children under five.
It is clear that wholesale reliance on any of these solutions is wildly unsustainable, and that Kenyans need a long-term solution for our universal healthcare that is designed for our unique needs instead of adopting the detailed, complex issues of other nations.
While it may be tempting to hurriedly assemble an alarmist response to the crisis at hand, the doctors on strike themselves remind us that careful assessment and implementation of customised policies is the only way to quality public healthcare in Kenya. Let us, therefore, continue the good fight of national dialogue and protest not only because it is radical and visionary, but because it is essential.
 The Standard Group Plc is a
multi-media organization with investments in media platforms spanning newspaper
print operations, television, radio broadcasting, digital and online services. The
Standard Group is recognized as a leading multi-media house in Kenya with a key
influence in matters of national and international interest.
The Standard Group Plc is a
multi-media organization with investments in media platforms spanning newspaper
print operations, television, radio broadcasting, digital and online services. The
Standard Group is recognized as a leading multi-media house in Kenya with a key
influence in matters of national and international interest.