×

The Standard e-Paper
Kenya’s Boldest Voice
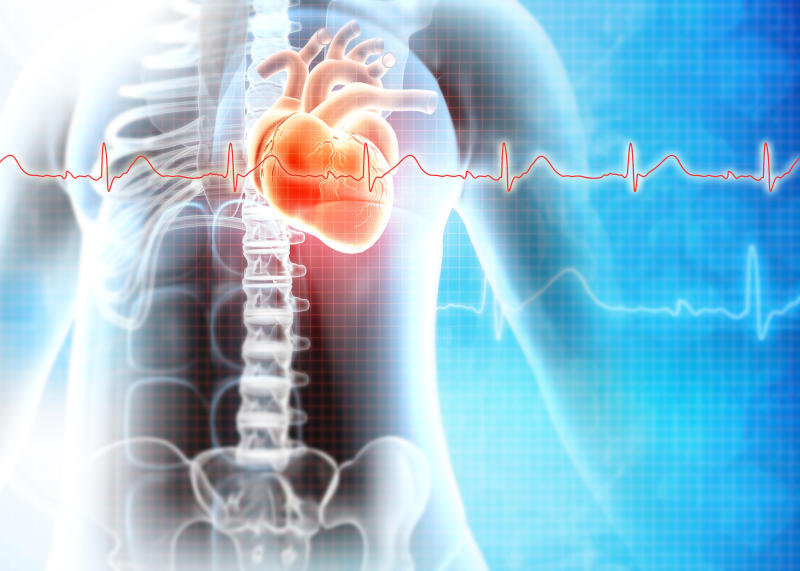
Cardiovascular disease (CVD), including heart disease and stroke, is the world’s number one killer. According to the World Heart Federation, cardiovascular disease kills 17.5 million people each year. This is expected to hit 23 million by 2030. In Africa, the latest projections suggest that by 2030, more people will die from coronary artery disease than from any other cause. This is attributed to increased urbanisation, lack of preparedness and unhealthy lifestyles.
Subscribe to our newsletter and stay updated on the latest developments and special offers!