×

The Standard e-Paper
Stay Informed, Even Offline
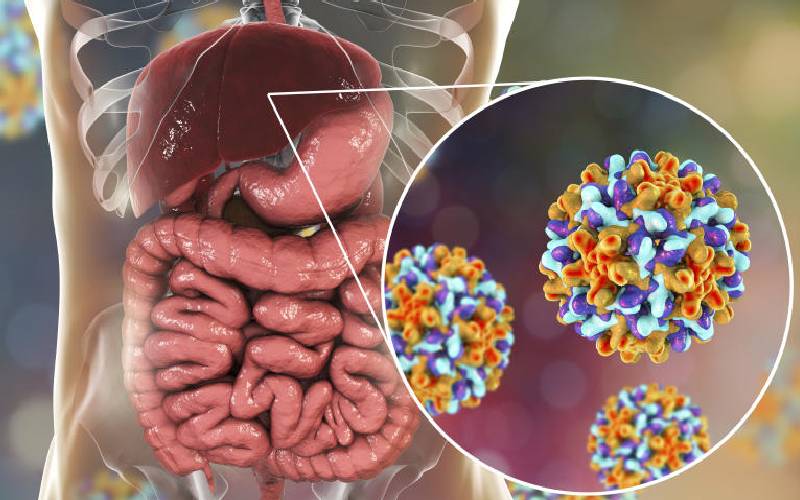
It started as a mild discomfort accompanied by diarrhoea that just refused to go away, even with medication.
Subscribe to our newsletter and stay updated on the latest developments and special offers!