The Standard Group Plc is a
multi-media organization with investments in media platforms spanning newspaper
print operations, television, radio broadcasting, digital and online services. The
Standard Group is recognized as a leading multi-media house in Kenya with a key
influence in matters of national and international interest.
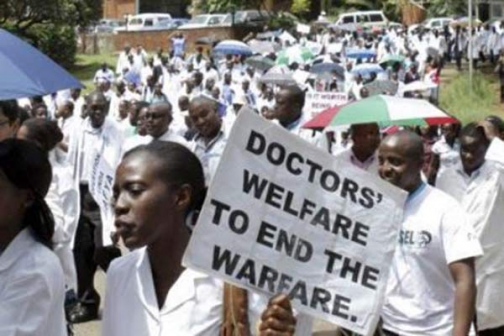
Many doctors and patients are cognizant of the fact that locally, the national rationale of only responding to patient or worker complaints during crisis thrives even in private facilities. Further to this, prices and qualities of care vary so widely between facilities and service providers that it is difficult to reliably project treatment costs, especially in the case of chronic conditions.PHOTO:COURTESY
The nation spends a lot of time bemoaning the brains that carry our best minds and talents away from the public health sector.
Eighty per cent of Kenyan doctors reportedly leave the civil service either for private practice locally or across the borders to work for public or private health care sectors abroad. This means that for every five doctors trained in Kenya, the public sector is only able to retain one despite the urgent need for trained personnel.
Premium Article
Get Full Access for Ksh299/Week.
Fact-first reporting that puts you at the heart of the newsroom. Subscribe for full access.
🔥 Flash Sale !
Subscribe now and enjoy 50% off monthly and annual plans. Offer ends in…
Stand With Bold Journalism.
Stand With The Standard.
Journalism can't be free because the truth demands investment.
At The Standard, we invest time, courage and skills to bring you accurate,
factual and impactful stories. Subscribe today and stand with us in the
pursuit of credible journalism.